“Thank you for saving my life, and thank you to all the medical staff.” Recently, the Rheumatology Department of Renji Hospital, affiliated with Shanghai Jiao Tong University School of Medicine, received a special token of gratitude. In a video message, patient Lao Hua (pseudonym), seated in a wheelchair, reflected emotionally, “From being completely bedridden and immobile to now sitting here and speaking, I’ve cheated death twice.”
Three months prior, Lao Hua was diagnosed with squamous cell carcinoma of the right lung. He underwent anti-tumor chemotherapy combined with anti-PD-1 immunotherapy. However, just one treatment cycle later, he developed severe systemic weakness, breathing difficulties, and even lapsed into a coma. These life-threatening symptoms were caused by a severe adverse reaction to the immunotherapy. During his three-week treatment at Renji Hospital, the department’s “Dr. House” team employed precise targeted intervention, life support, and meticulous rehabilitation, enabling Lao Hua’s recovery.
The severity of this immunotherapy reaction was completely unexpected for Lao Hua and his family!
His family informed reporters that at the local hospital, Lao Hua had required emergency resuscitation and endotracheal intubation. Tests showed significantly elevated creatine kinase levels, and electromyography (EMG) indicated a mixed pattern of muscle damage. However, myositis-specific antibodies and myasthenia gravis antibodies were both negative. High-dose glucocorticoids and immunomodulatory therapy proved ineffective. The cause of his severe myositis remained undiagnosed! Dependent on mechanical ventilation, his life hung in the balance. Through remote consultation, Dr. Li Ting, Associate Chief Physician of Renji Rheumatology, identified the likely culprit behind Lao Hua's systemic muscle weakness: a severe adverse reaction triggered by the anti-tumor immunotherapy.
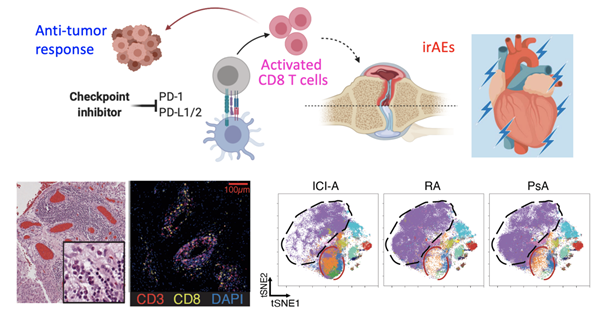
Clutching at hope, Lao Hua's family brought him to Shanghai Renji Hospital. Under the coordination of Associate Chief Physician Dr. Wang Xiaodong, the Rheumatology Intensive Care Unit rapidly conducted a multi-system, multi-dimensional assessment encompassing his muscular, immune, neurological, and respiratory systems. Immunological testing confirmed the presence of immune checkpoint inhibitor-associated adverse events (irAEs). The immunotherapy had caused excessive activation of effector T cells, damaging skeletal and respiratory muscles throughout his body and resulting in a state mimicking "total paralysis."
Leveraging their research expertise in immunotherapy toxicity, Rheumatology Department Director Dr. Ye Shuang and the ICU team devised a treatment plan for Lao Hua involving targeted intervention, life support, and meticulous rehabilitation. They initiated therapy with abatacept, a CTLA-4 fusion protein, to counteract the muscle inflammation and tissue damage caused by the immune system's overactivation.
Through the close collaboration of Drs. Chen Zhiwei and Wang Runci in the Rheumatology ICU and the nursing team, Lao Hua's creatine kinase and inflammatory markers began to normalize. His muscle strength gradually returned, and his dependence on the ventilator decreased. After three weeks, he was successfully discharged to a rehabilitation hospital. Following two weeks of intensive rehabilitation, Lao Hua was finally weaned off the ventilator, had his feeding tube removed, and regained the ability to breathe and eat independently.
In the renowned medical drama House M.D., Dr. House consistently unravels diagnostic mysteries through deep medical knowledge and advanced assessment, miraculously curing complex illnesses. Similarly, Renji Rheumatology's “Dr. House” team is pioneering the treatment landscape for adverse reactions to anti-tumor immunotherapy.
While immunotherapy offers significant hope for many cancer patients by enhancing immune function to fight tumors, the adverse events stemming from immune checkpoint blockade demand serious attention. Dr. Ye Shuang emphasized that the activated immune system can also indiscriminately attack the patient's normal cells and tissues. Inevitably, some patients develop irAEs such as autoantibody abnormalities, rashes, myositis, arthritis, and pneumonitis. “The critical factor is whether we can recognize these reactions and devise solutions; no matter how these adverse events evolve, we aim to maintain control.”
Over the past four years, Renji Hospital's Rheumatology Department has established a dedicated clinical cohort for studying irAEs. Collaborating with leading teams from Harvard University, Cornell University (USA), and Sorbonne University (France), they have conducted in-depth research into the pathogenic mechanisms and immunological signatures of these adverse events. They have proposed stratified treatment strategies targeting specific cytokines and immune cells, developing a set of precise and effective protocols for assessment, diagnosis, and treatment. These efforts have significantly improved the prognosis for patients experiencing severe irAEs related to anti-tumor immunotherapy.