A 53-year-old man presented with an 8-year history of recurrent odynophagia and oral ulcer. The first esophagogastroduodenoscopy (EGD) was initially performed at 2015, but we could not know the detailed description. The past medical record retained by the patient showed that the earliest EGD report we could read was performed in Oct-2019 at a local hospital, revealing a 0.4*0.5cm ulcerated esophagus lesion along with protruding mucosa around. At that time, electronic colonoscopy showed superficial small ulcer of terminal ileum. The results of pathologic examination showed acute activity of chronic mucosal inflammation. CT of chest showed scattered small nodules in the lungs. With the history of oral ulcers, the patient was diagnosed with Behcet's disease in local hospital. He had taken prednisolone, thalidomide and sulfasalazine monotherapy or combination therapy, without good response. He also underwent therapy for eleven months due to suspected pulmonary tuberculosis (tbc) (HRE, isoniazid + rifampicin + ethambutol). An EGD was performed in Jul-2021, showing two ulcerated esophagus lesions, with expanded range compared with that in Oct-2019.
In Jun-2023, he presented to our hospital because of recurrent oral ulcer and odynophagia. An EGD revealing a 1.0*0.5cm protruding (Fig.A) with ulcerated lesion in the middle, and another submucosal protrusion with ulcerated lesion in the lower esophagus (Fig.B). Electronic colonoscopy showed no significant lesion. The T-SPOT was positive (A 37, B 68). The HLA-B genotype was tested negative for Behcet's disease. Further workup, including tumour markers, and test screening for autoimmune disease, viral, bacterial and parasitic infections were all within normal limits. CT of chest showed scattered small nodules in the lungs. CTE showed non-specific prompt. Esophageal tuberculosis must be considered, we advise diagnostic anti-TB therapy. The patient took PaRftEZMfx for anti-TB treatment for two months, followed with PaRft for one month. An EGD was performed after three-month treatment, showing a 0.5*0.5cm protruding (Fig.C) and the ulcerated lesion was healed (Fig.D). And the oral ulcer also disappeared, along with the clinical symptoms. Anti-TB therapy was suggested to be continued. This case was published on Digestive Diseases and Sciences(2024, 69:2715–2716).
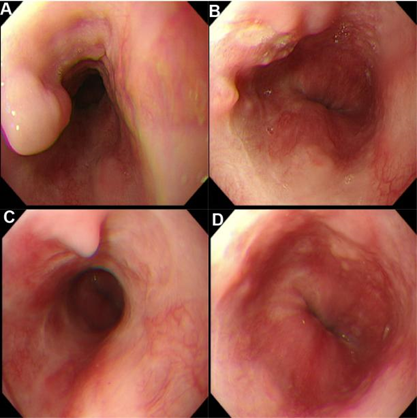
Fig. 1 Endoscopic view before (A, B) and after tbc therapy (C, D).